-
Muñoz OM, Rodríguez NI, Ruiz Á, Rondón M. Validación de los modelos de predicción de Framingham y PROCAM en una población colombiana. Rev Colomb Cardiol. 2014;21(4):202–212.
paper -
Hageman SHJ, McKay AJ, et al.. SMART2 risk prediction algorithm. Eur Heart J. 2022;43(18):1715–1727.
paper -
Mancini GBJ, Ryomoto A. Adoption of the PREVENT Risk Algorithm: Potential International Implications. JACC Adv. 2024;3(8):101122.
paper -
Scheuermann B, Brown A, et al.. External Validation of the AHA PREVENT Cardiovascular Disease Risk Equations. JAMA Netw Open. 2024;7(10):e2438311.
paper -
WHO CVD Risk Chart Working Group. WHO CVD risk charts: revised models for 21 global regions. Lancet Glob Health. 2019;7(10):e1332–e1345.
guideline -
Collins GS, Moons KGM, et al.. TRIPOD+AI statement. BMJ. 2024;385:e078378.
standard -
Liu T, Krentz A, Lu L, Curcin V. ML-based prediction models for CVD risk using EHR data: systematic review and meta-analysis. Eur Heart J Digit Health. 2024;6(1):7–22.
paper -
Damen JA, Pajouheshnia R, et al.. Performance of the Framingham risk models and pooled cohort equations. BMC Med. 2019;17(1):109.
paper -
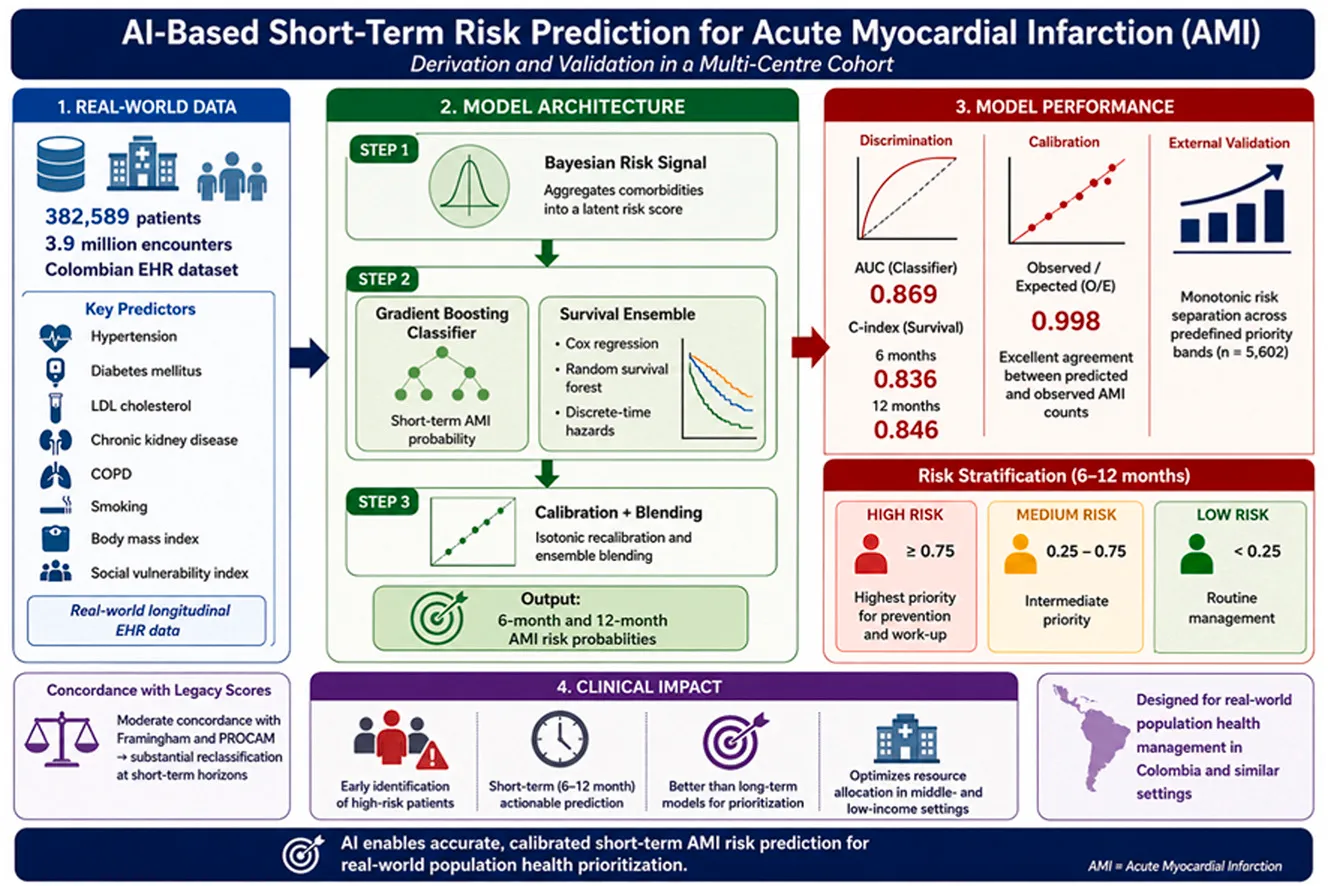
Amorocho-Morales JD, Parra-Guevara S, Quintero-Muñoz E, Dimas G, Correa-Morales JE. A next-generation prediction risk model for acute myocardial infarction: Derivation and validation in a multi-centre cohort. Int J Cardiol Cardiovasc Risk Prev. 2026;30:200659. doi:10.1016/j.ijcrp.2026.200659.
paper -
Krittanawong C, Virk HUH, et al.. Machine learning prediction in cardiovascular diseases: meta-analysis. Sci Rep. 2020;10(1):16057.
paper -
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613.
DOI →
-
Cassiani-Miranda CA, Cuadros-Cruz AK, et al.. Validity of the Patient Health Questionnaire-9 (PHQ-9) for depression screening in Colombia. Rev Colomb Psiquiatr. 2020.
DOI →
-
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097.
DOI →
-
García-Campayo J, Zamorano E, et al.. Cultural adaptation into Spanish of the GAD-7. Health Qual Life Outcomes. 2010;8:8.
DOI →
-
Remor E. Psychometric properties of a European Spanish version of the Perceived Stress Scale (PSS). Span J Psychol. 2006;9(1):86–93.
DOI →
-
Molinero Ruiz E, Basart Gómez-Quintero H, Moncada Lluis S. Validation of the Spanish version of the Copenhagen Burnout Inventory (CBI). Rev Esp Salud Publica. 2013;87(2):165–179.
DOI →
-
King M, Walker C, et al.. Development and validation of an international risk prediction algorithm for episodes of major depression (predictD). Arch Gen Psychiatry. 2008;65(12):1368–1376.
DOI →
-
Moreno-Peral P, Luna JD, et al.. Predicting the onset of anxiety syndromes at 12 months in primary care (predictA). PLOS ONE. 2014;9(9):e106370.
DOI →
-
Fernandez A, Salvador-Carulla L, et al.. Development and validation of a prediction algorithm for the onset of common mental disorders (HILDA). Aust N Z J Psychiatry. 2018;52(1):47–58.
DOI →
-
Inoue S, et al.. Predicting mental health–related sick leave using stress check data. J Occup Health. 2026;68(1):uiag011.
DOI →